Many of the people that we engaged with had very poor experiences of being in hospital. This ranged from an unsatisfactory physical environment through to racism on the part of staff. Some felt unsafe in closed environments, having been shouted at and intimidated by staff. Others had experienced physical restraint, seclusion or forced medication. People told us that ward environments did the bare minimum to ensure the wellbeing of patients.
Discharge from hospital was difficult for people in a number of ways with many feeling both unsupported and unprepared. From our engagement with people, recurrent issues were highlighted with aftercare – many felt they did not get enough support after they left hospital. This was especially true for people with multiple needs such as homeless people, who faced the double-edged sword of needing housing provision in addition to support with maintaining their mental health.
People told us there was a lack of communication around leaving hospital. Some felt that they were discharged too soon and in select cases that this decision was made unfairly, whereas others believed that they stayed in hospital too long.
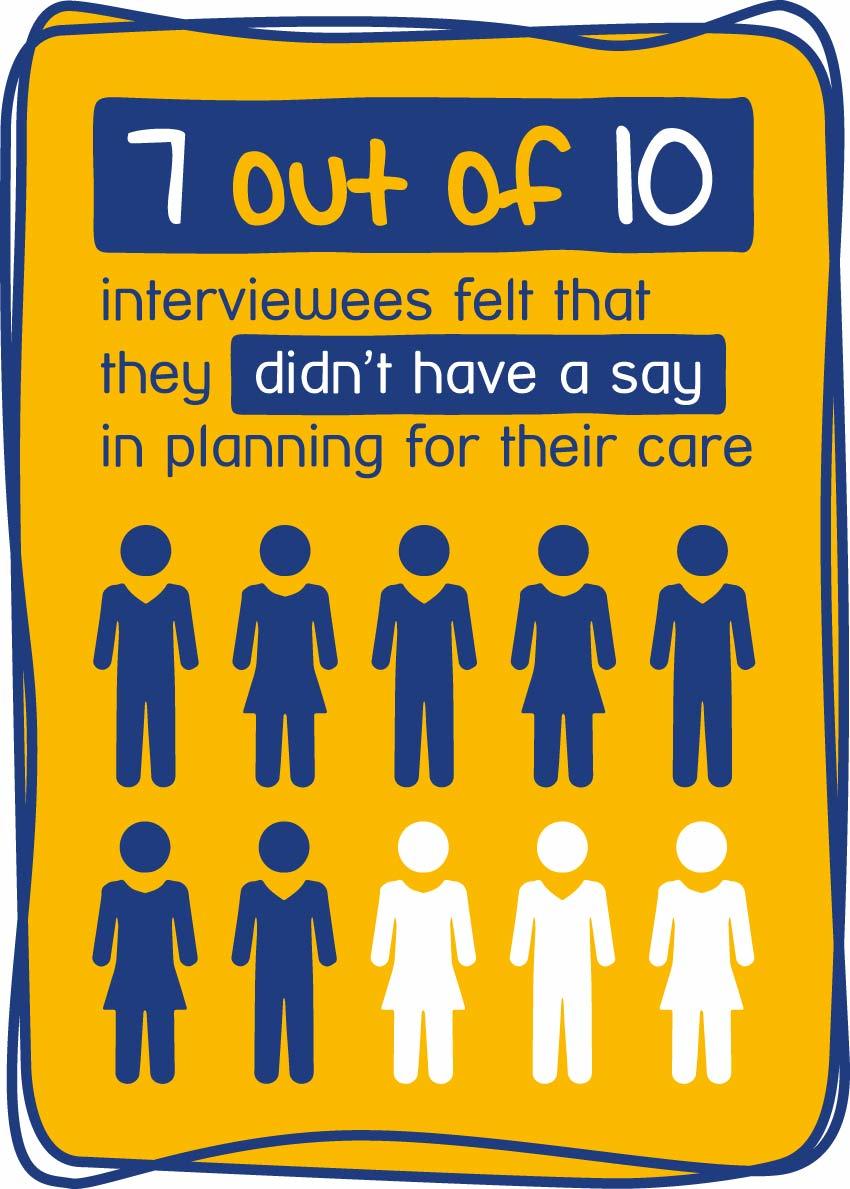
Experiences with care planning differed among the people we engaged with. Some people had very positive experiences with care plans, but most people did not. While we did hear about some good examples of care plans which helped to facilitate recovery, it was disheartening to hear that many of our participants did not have care plans and those that did had very little involvement in writing their care plan. One of the participants shared that it was almost inevitable to slip back into the ‘system’ when there is no care plan and no co-ordination between hospitals and community services.
Participants from our telephone interviews told us they felt ignored and misunderstood by staff while in hospital, with little opportunity to have a say about their care. Some suggested that greater access to advocacy (getting support from another person to help you express your views and wishes, and help you stand up for your rights) would be helpful when speaking to professionals, so they could have more meaningful involvement in their care. Additional suggestions for improvement were for staff to be better equipped to provide more culturally and religiously sensitive care.
A CTO is an order made by a clinician which allows someone to be treated in the community for their mental health, instead of staying in hospital. But they can be called back to hospital and given immediate treatment if necessary.
Black and Black British people are over eight times more likely to be on a CTO than White people . Black participants in our engagement suggested the reason for this disproportionate use was that Black people were not trusted to adhere to treatment and take medication, so clinicians used CTOs as a form of surveillance.