Reducing health inequalities for people with mental health problems
It also affects your experiences of getting treatment and support. And, shamefully, those of us with severe mental health problems are still likely to die 16-20 years earlier than the general population. This needs to end.
We know that Black or black British people are four times more likely to be detained under the Mental Health Act than white people. Meanwhile, black British people are eight times more likely to be out on a Community Treatment Order (CTO).
Black and minority ethnic (BAME) people also report worse experiences and outcomes from services and are more likely to be restrained. There are many reasons for this including discrimination, deprivation and structural racism, stigma and stereotyping.
People from LGBTQ+ communities also have disproportionately high levels of mental health problems. They are more likely to self-harm and have suicidal thoughts, and often have poor experiences of mainstream services.
Women report poor experiences of a mental health system that doesn’t consider their experiences of violence, abuse and trauma.
People with complex needs (for example people with a mental health problem or a drug or alcohol problem) often experience multiple discrimination and fall into the gaps between services. And people with mental health problems smoke 42 per cent of all cigarettes, with smoking rates much higher than the general population.
Finally, there we know that some diagnoses are more stigmatised than others and we need to do much more to ensure has been a woeful response to supporting the needs of people such as those with with personality disorders, have given their poor much better experiences and outcomes.
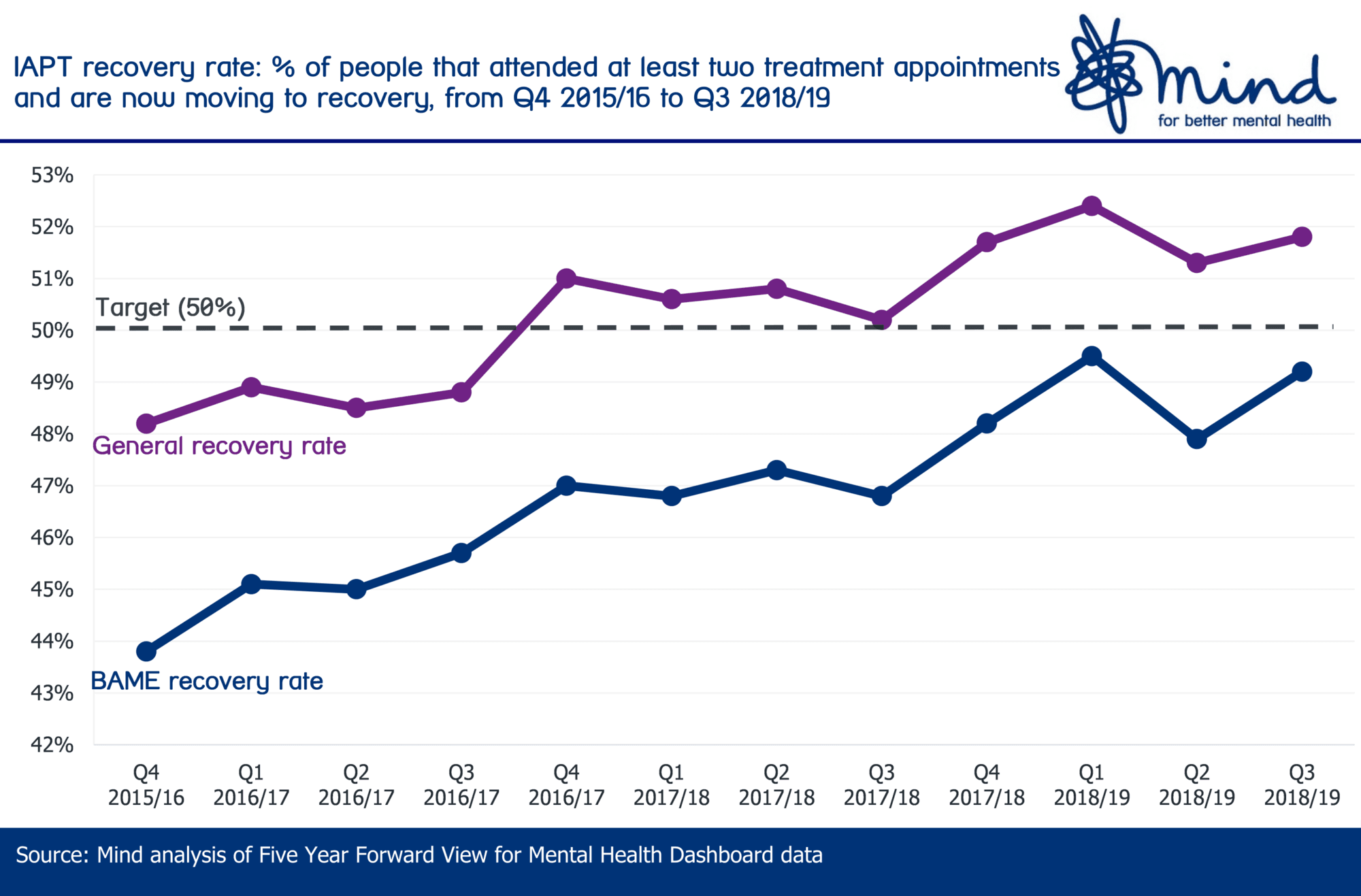
People from BAME backgrounds are less likely to recover after using IAPT services than the general population.
The Mental Health Act Review sets out how mental health services can continuously engage with BAME groups through an Organisational Competency Framework (OCF). This ensures services are designed and delivered to reflect the needs and preferences of the local community. It also calls for the introduction of culturally competent advocacy and a more diverse workforce with people from Black African and Caribbean backgrounds represented at all levels of the mental health professions.
The NHS should develop different service models, such as online and face-to-face peer support and mentoring. It should also develop partnerships with voluntary and community sector services that have extensive experience of supporting disadvantaged groups.
The Women’s Mental Health Taskforce has set out what national bodies and service providers can do to take a gender- and trauma-informed approach. This has been picked up in the plans to reshape primary and community mental health services. We’re waiting for the next steps from government on the other recommendations.
The NHS and wider services must learn from successful initiatives such as the Making Every Adult Matter (MEAM) approach to coordinating care for people with complex needs.
We welcome the long-term plan’s commitment to offer smoking cessation to people in contact with specialist mental health services. These services need to be tailored to the needs of people with mental health problems and geared to helping people to develop healthy coping strategies.
People with Personality Disorders need better support. The Consensus Statement on Personality Disorders provides a blueprint on action to ensure people with personality disorder are no longer left behind.
Every system plan must show how local areas will address key health inequalities and how additional funding is targeted to disadvantaged and vulnerable groups. This includes people with disabilities, LGBTQ+ and BAME communities. System plans must take account of the patient and carers race equality framework (PCREF) NHS England is developing.
A new universal smoking cessation offer will also be available as part of specialist mental health services for long-term users and in learning disability services. This will include the option to switch to e-cigarettes while in inpatient services.
Is your plan ambitious enough in tackling the health inequalities faced by people with mental health problems?
Is the local system working with the voluntary and community sector to reach groups who experience the worst health inequalities?
Does the plan include ensuring better take up of health checks and follow-up care for people with severe mental illness and tailored smoking cessation for people in contact with specialist mental health services?
Is your plan seeking to address race equality when delivering services and within the workforce?